BY WAYNE LEWIS
Scientists in the Keck School of Medicine of USC’s Department of Population and Public Health Sciences are stepping up to evaluate climate change’s impact on human health — particularly for communities already enduring disparities — and devise ways to reverse course. Within the last few years, a cadre of four faculty members concerned with the detriments of air pollution have expanded their research to encompass climate change:
Erika Garcia, PhD, MPH, assistant professor in the Division of Environmental Health
Rima Habre, ScD, MSc, associate professor (clinical) in the Division of Environmental Health and the Spatial Sciences Institute
Jill Johnston, PhD, associate professor and director of community engagement in the Division of Environmental Health and the Spatial Sciences Institute
Rob McConnell, MD, professor in the Division of Environmental Health
In a recent group conversation, these researchers discussed why and how they do what they do, what their studies are beginning to find, and what can be done to mitigate the climate crisis and safeguard human health.
How did each of you come to study climate change and human health?
Erika Garcia: As public health professionals, we’re drawn to an area of need, and climate change is this huge challenge that everyone in the world will be affected by to various degrees.
Jill Johnston: For me, it came out of my own experience. Living in Texas, I was affected by the oil industry and seeing the impacts of climate change. I got involved as a youth in community organizing, working on addressing climate justice within the U.S. and climate policy at a local and international level. Later in life, I brought this experience to academia.
Rima Habre: I’ve always been interested in understanding environmental exposures and specifically air pollution. I worry about how much heat stress we’re all experiencing, as well as air pollution and wildfire smoke — that’s way more prominent these days. Add to that my work around environmental health disparities, and that’s what drew me into wildfire-focused climate research.
“With urban heat islands, lower–income individuals in these concrete jungles aren’t getting the same cooling effects that other people have, so their health conditions are exacerbated.”
Rima Habre, ScD, MSc
Rob McConnell: For many years, we worked on a big project called the Children’s Health Study, a longitudinal study of air pollution and health effects in children. About 15 years ago, we started to estimate the burden of disease. It gets policymakers’ attention to say, “We’re killing people with air pollution.”
I think climate change can follow the same model. It hasn’t been that concrete for people until recently. In Southern California, we can expect drought and a big increase in extreme heat waves, in addition to the wildfires Rima mentioned. There are going to be all kinds of health effects, and putting real numbers on those effects is one way to engage people.
Climate change is a global problem, but it seems that it may hurt some populations more than others. What disproportionate effects are you seeing in underserved communities?
EG: In one of our studies, we’re looking at the impact of heat on risk of mortality in California. Thinking about possible interventions, we have data on air conditioning use, and we see that A.C. use is related not only to whether an area is hotter or colder, but also to average income and other measures of socioeconomic status. We are still trying to understand how A.C. access impacts risk of death from heat. But something we see across the board for a variety of health exposures and outcomes is that there are disparate impacts in vulnerable communities.
There’s been a movement in the last few years to think about larger structural, social factors that are driving forces behind certain disparities in resource access and exposure. Those things don’t exist in a vacuum; they’re a product of our society. So we try to figure out how to best capture that in our analyses.
“Most people don’t want to read academic journal articles, but people do want to know the information.”
Jill Johnston, PhD
RH: Climate, heat, temperature and wildfires can be very broad regional exposures, but they can also have strong local impacts. When we think about neighborhoods, and the social factors that Erika talked about, you often see that one specific group gets an overload. For example, with urban heat islands, lower-income individuals in these concrete jungles aren’t getting the same cooling effects that other people have, so their health conditions are exacerbated.
The same goes for where we place our parks and how we build our cities. That’s where geospatial thinking and modeling comes into play: We model neighborhoods and the co-occurrence of risk factors. But also, at the most individual level, we think about where people spend their time. Are they indoors? Do they have access to quality parks, cooling centers, medical services?
RM: Just to emphasize what Erika and Rima said, if you look at a map of greenspace in Los Angeles, you see a lot of green in affluent areas. But if you go to South Central, there’s not a lot of green there. That puts people at risk right away for extreme heat events. And it’s worse if they can’t afford air conditioning. Many different factors conspire against these vulnerable communities.
JJ: There’s a whole global context and issues of global equity, and I want to acknowledge that. But particularly thinking about communities in the U.S. — which is responsible for the majority of greenhouse gas emissions — communities situated next to the fossil fuel industry are affected directly by the pollution. And those same communities are going to be first and most affected by climate change. This is predominantly in communities of color, in spaces that have the fewest resources and the least amount of political power to affect this.
Can you tell me a little bit about the secret sauce in each of your research programs — interesting approaches that people may be unaware of?
EG: There’s a way of thinking called a counterfactual framework. For example, here is the current setup for greenspace in our communities. But in an alternative reality, everything else being the same, what if parks were placed differently? You have these two different realities, one of them you observed and one you didn’t, and we try to estimate what would have happened under these different scenarios.
“Southern California is a particularly good laboratory for getting a handle on fossil fuels, because we were the original 20th century sprawling city.”
Rob McConnell, MD
Of course, we don’t have alternative realities. We use a lot of modeling and different kinds of data science approaches, such as machine learning, to tie the unreal back to the real, using our observational data. It’s part of thinking about real-world solutions and having the science to understand what may happen with our interventions.
RM: I think of it as, “Just imagine.” The world doesn’t have to be what it is. To me, that’s a powerful concept.
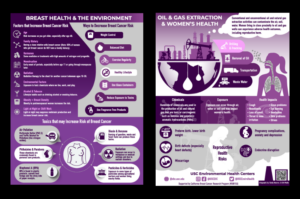
JJ: We’ve worked to synthesize complex health research in ways that are easily accessible and culturally relevant to a lot of the communities here in Southern California. Most people don’t want to read academic journal articles, but people do want to know the information.
Using infographics, with a lot of visuals backed up by evidence, has been an effective tool in engaging communities to digest the science, as well as in talking to policy makers.
RH: To me, there’s two things. One is data visualization and mapping, using colors and storytelling with actual data. Part two is this precision environmental health approach where I deploy all these gadgets: GPS monitoring, wearable sensors for millisecond-level measurements of personal air pollution exposure, devices that measure ultrafine particles or gases, and others that collect particles on filters for chemical analysis. We get to see what is going on at very high resolution.
What does everyone need to know about climate change and health?
JJ: We don’t have to take on this problem globally. We can think about what’s in our backyard. For an audience that’s here in Southern California, L.A. is the largest urban oilfield in the country. There’s active oil extraction every day. We can do a lot of things locally to phase out use of fossil fuels, address the climate emergency and develop resilience in communities.
“There’s also the idea of co-benefits. You can improve one thing, but also get benefits from another angle.”
Erika Garcia, PhD, MPH
EG: We need a multipronged approach, intervening at multiple levels from different angles. In our department, we work with folks in environmental engineering, urban planning, social work and architecture. This transdisciplinary approach helps us identify potential interventions that can be applied at different levels — and do the science to show whether they have benefits.
There’s also the idea of co-benefits. You can improve one thing, but also get benefits from another angle. With Jill’s example, if we reduce or eliminate the need for oil wells in Los Angeles, that will generate less greenhouse gases. But there’s also a health benefit for local community members, who are no longer going to be exposed to fugitive emissions from those wells. A lot of the things that we know will reduce greenhouse gases also have health co-benefits.
RM: Jill and I just received support from the National Institutes of Health to create the Southern California Center for Children’s Environmental Health Translational Research. The idea is to take what we know about the environment and health, and apply it to education that will result in change. Our theme is, “Imagine a Los Angeles without fossil fuels.”
Southern California is a particularly good laboratory for getting a handle on fossil fuels, because we were the original 20th century sprawling city — an urban experiment gone wrong starting in the 1940s and ’50s, turning Southern California into a place where you couldn’t do anything without getting in your car. If we can fix this problem, then anybody can.
But it’s going to involve redesigning the city so that people have more access to jobs near their house, better public transportation and local commerce that they can get to without cars. It’s a big challenge. Beyond climate change, there are the co-benefits of better health and a better city to live in.
Jill has developed something really neat: We’re not just working with our usual colleagues in health and the hard sciences. We’re talking to scholars in the humanities, who think about how to communicate things so that people respond, in a way that they don’t respond to just numbers. It’s an exciting new approach for engaging communities, and empowering them to make their own decisions and to require their representatives to make decisions that are in their interest.
JJ: One of the exciting pieces is that this center is going to focus on solutions. A lot of our work has just been about documenting problems. Coming at it with this interdisciplinary approach, in partnership with communities, we’re hoping we can leverage all the community organizing, add some data and art, and hopefully help advance policy at a local level.
RH: In some of our studies of pregnant women and environmental health disparities, we’re doing this very high-resolution GPS tracking and measurement of what people are actually breathing. And the more greenspace they encounter, it’s directly associated with a huge decrease in their personal exposure to air pollution. To me, that’s striking.
Adding more parks has co-benefits. People can exercise — with direct health benefits as well as mental health benefits that we’ve seen clearly, especially with COVID — but also less greenhouse gases, removal of air pollution, lower noise, all sorts of things. Like Rob said, we need to do a better job as scientists communicating local impacts and benefits.
We spoke about solutions. What would be your personal favorite?
RH: To me, it’s just more nature, greenness and ecological biodiversity. Increasing contact with nature is a simple solution that’s so multipronged, with so many co-benefits.
EG: Thinking of the health disparities we can expect to see, I’m going to say we need to focus on poverty and everything that goes with it. There are barriers that exist more for some people than for others because of structural inequities. That is a huge driver of disparities.
We need to think bigger. How do you intervene on poverty? It’s a big question. But because it is big, we cannot ignore it.
JJ: I want to start with my least favorite solution: buying our way out of climate change, such as getting a new, fuel-efficient car. That’s strictly tied to an individual’s purchase power. Instead, it’s important for communities to think about how taking the bus to work every day is an act that supports climate justice.
In terms of a big-picture policy direction, I would just point to all the work that has been done at the county and the city level to move toward phasing out fossil fuel extraction in L.A. County. We need to transition from using fossil fuels to building the green economy and a green workforce.
RM: Fairly recently, I got interested in the health care industry’s carbon footprint — it’s enormous. Health care accounts for about 8 to 10% of the total U.S. greenhouse gas emissions. There’s a growing movement to address the carbon footprint of the healthcare industry and to lead by example. It’s a great place for us to start.
That involves simple things such as getting rid of anesthetic gases that have a huge climate impact; electrifying our vehicle fleets; supplying our own electricity, especially in Southern California where there’s a lot of sun; and creating less waste — in particular disposable equipment and supplies — because waste comes with a carbon footprint. As a big medical center, we could have an outsize impact on reducing emissions, on equity, and on the quality of life in our communities by hiring and purchasing locally.
For more about Earth Week panels, events and social media initiatives, visit the USC Office of Sustainability.